
About the Author:
Jeff Nunn is the founder of Project Biohacking. With over 30 years of biohacking practice, he applies decades of self-experimentation methodology to peptide research, dosing math, and vendor evaluation.
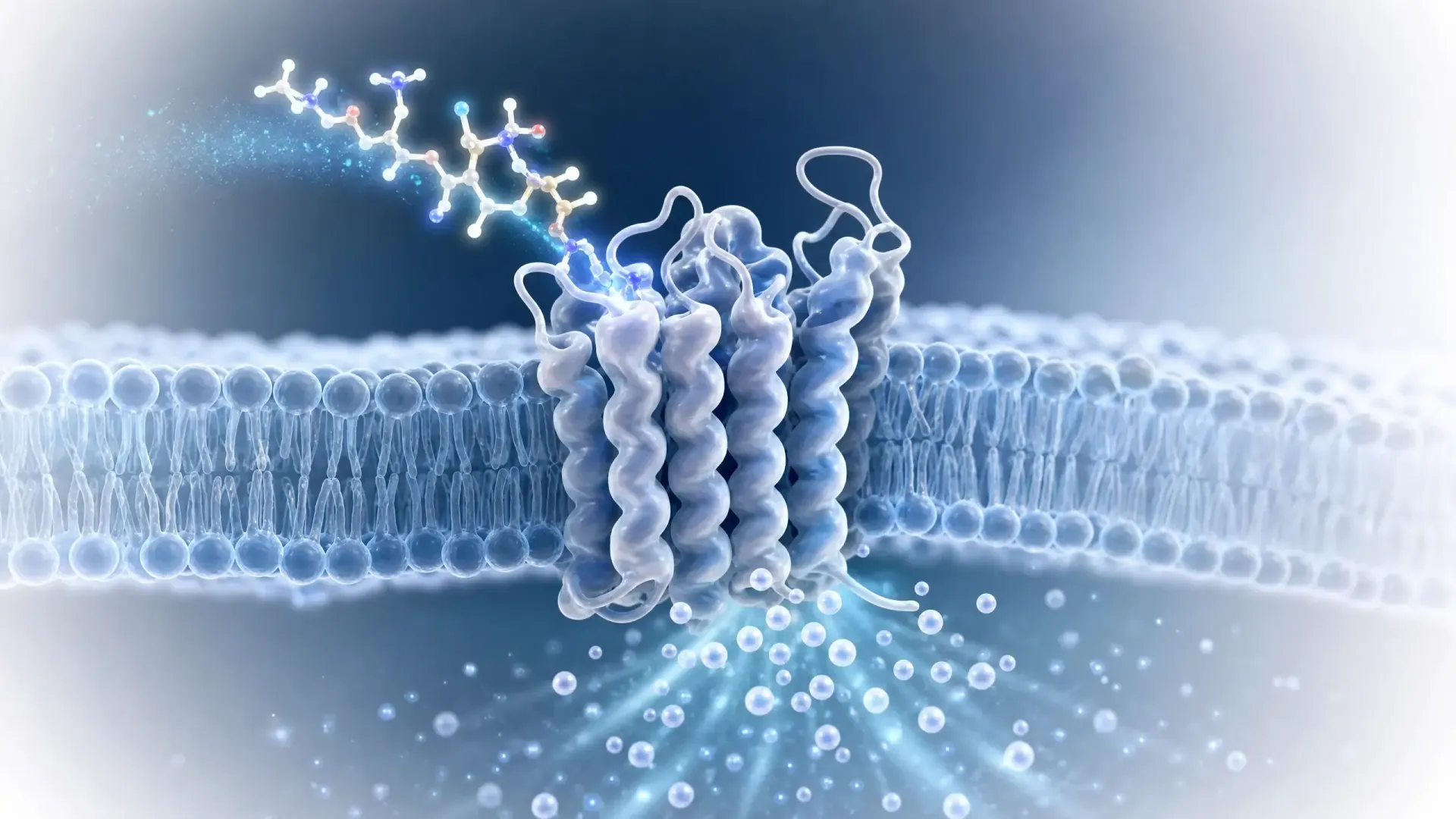
Oxytocin peptide is a nine-amino-acid neuropeptide your body makes in the hypothalamus and releases from the posterior pituitary gland. Most people know it as the "bonding hormone," but that label barely covers what this small peptide does across social behavior, stress, reproduction, appetite, and even pain. This guide covers what oxytocin peptide does, how it works, what the research shows, how it is used intranasally, and the side effects that matter most.
Oxytocin is a nonapeptide, a molecule built from a chain of nine amino acids. Your body makes it in the hypothalamus, inside large neurons in two clusters called the paraventricular and supraoptic nuclei. Those neurons run down to the posterior pituitary gland, which stores the peptide and releases it into the blood.
It plays two roles at once:
The oxytocin used in hospitals is a synthetic copy of this same peptide, given by IV to start or strengthen labor and to control bleeding after birth. That clinical use is tightly controlled, and it sits apart from the experimental, off-label interest that draws biohackers to oxytocin as a peptide. If you are new to the category, our primer on what peptides are covers the basics, and peptide therapy explains how these compounds get used more broadly.
The split between a body hormone and a brain signal starts at the receptor.
Oxytocin binds the oxytocin receptor, a G-protein coupled receptor. Once it binds:
In the brain, oxytocin works differently. It shifts activity in regions like the amygdala and the nucleus accumbens, which handle emotion and reward. That is the basis for its reputation around trust, empathy, and reading social cues.
Oxytocin secretion is not constant. The body releases it in response to specific cues:
Knowing the mechanism is not the same as knowing the effect, and the evidence is stronger in animals than in people.
Most human work uses a single intranasal dose and measures social cognition. Across these studies:
The clearest mechanistic picture comes from ethology, the study of animal behavior. Across mammals, oxytocin shapes how animals recognize, bond with, and communicate with each other:
Almost all of the deep mechanistic data comes from animals, from mice and rats to voles, sheep, and monkeys, not from people. The jump from an animal model to a human is not small, and it is the main reason human results look weaker than the rodent picture.
Because oxytocin shifts social perception, researchers have studied it in conditions where social or emotional signaling is affected. That work spans autism, schizophrenia, generalized social anxiety, and alcohol use disorder, where early trials in patients have looked at whether oxytocin changes social skills, fear responses, or craving. The results are early and often conflicting, which is the honest state of this evidence.
Oxytocin's reach goes past bonding, which is why interest in it keeps widening into appetite, muscle, and pain.
Oxytocin helps regulate appetite, eating behavior, and body weight, and it interacts with how the body handles blood sugar.
One widely cited study found that blood oxytocin declines with age in mice, and that giving oxytocin to aged mice improved muscle regeneration by waking up muscle stem cells. The authors linked a genetic lack of oxytocin to early sarcopenia, the age-related loss of muscle. This is animal data. It says oxytocin physiology touches tissue repair, not that a nasal spray rebuilds muscle in people.
Oxytocin receptors sit on nerves in the trigeminal system, which carries pain from the face and head. Intranasal oxytocin can quiet those nerves and block the release of CGRP, a signaling molecule involved in migraine and cluster headache.
This is an active but early area, not a settled use.
The fact that oxytocin fails by mouth explains why the intranasal route dominates the research.
The nose offers a path that partly bypasses the gut and may carry some oxytocin toward the brain. It is not efficient. Only about 1 to 2 percent of an intranasal dose is absorbed, and results swing with spray technique, head position, and congestion.
In the research literature:
Injectable oxytocin is a separate story. It is a clinical drug for labor and bleeding, and it does not reliably reach the brain, so an oxytocin peptide injection is not a shortcut to the social effects people read about.
The safety picture splits along that same line between nasal research use and clinical injection.
At the doses used in intranasal studies, reported side effects are usually mild:
In these trials the side effect rate often sits close to placebo.
The serious risks come almost entirely from clinical intravenous use, not nasal sprays:
One point worth stating plainly: the contraindications for oxytocin center on obstetric situations and on cardiovascular caution during rapid IV use. It is not restricted the way some other compounds are for prostate or hormone-sensitive conditions.
For biohackers, the sensible guardrails are simple:
Oxytocin's oldest and best-understood roles sit in female physiology.
These effects run deeper in women's reproductive biology than in any other use case, which is why oxytocin shows up so often in that research. Our overview of peptide benefits for women puts it in context alongside other compounds.
Get the numbers right before anything else
Oxytocin research is reported in IU, and turning those figures into an actual concentration is not obvious math. The
Peptide Calculator does the conversion for you, so when you are reading a study or comparing formulations, you are working from exact numbers instead of guesses.
Oxytocin peptide is a nine-amino-acid neuropeptide made in the hypothalamus and released from the posterior pituitary gland. It acts as both a hormone, on the uterus and mammary glands, and as a brain signal tied to social bonding, trust, appetite, and stress.
It binds the oxytocin receptor, a G-protein coupled receptor. In the body this raises calcium inside the cell and contracts smooth muscle, driving labor and milk let-down. In the brain it shifts activity in emotion and reward regions like the amygdala and nucleus accumbens.
The body releases oxytocin in response to labor and suckling, both through positive feedback loops, and to social touch and emotionally charged moments.
Almost all behavioral research uses an intranasal spray, because oxytocin taken by mouth is broken down in the gut. The nose partly bypasses that, though only about 1 to 2 percent of a dose is absorbed.
The most common single intranasal dose in human studies is 24 IU, with published trials ranging from roughly 8 to 48 IU. These are research doses, not a recommendation, and the response is non-linear, so a higher number does not mean a stronger effect.
At intranasal research doses, side effects are usually mild, such as headache, nasal irritation, and nausea, often near placebo levels. The serious risks, including low blood sodium and blood pressure changes, come mainly from clinical intravenous use rather than nasal sprays.
Yes. Researchers are looking at oxytocin for appetite and eating behavior, including in Prader-Willi syndrome, for muscle maintenance in aging (so far in mice), and for headache and craniofacial pain through its effect on trigeminal nerves. These areas are early and results are mixed.
Not directly. Rodent and other animal work gives the clearest picture of how oxytocin shapes bonding, social memory, and even muscle repair, but human effects are more modest and less consistent, and most mechanistic detail still comes from animals.
About the Author:
Jeff Nunn is the founder of Project Biohacking. With over 30 years of biohacking practice, he applies decades of self-experimentation methodology to peptide research, dosing math, and vendor evaluation.
Important Disclaimer: The content on Project Biohacking is for educational and informational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your health regimen, starting new supplements, peptides, or protocols. Nothing on this site establishes a doctor–patient relationship, and you use the information at your own risk. Research compounds discussed here are sold for laboratory research purposes only and are not approved for human or veterinary use or consumption.
“For educational use only. Not medical advice. Read our full disclaimer.”
+1 214-278-4039
All Rights Reserved | Project Biohacking